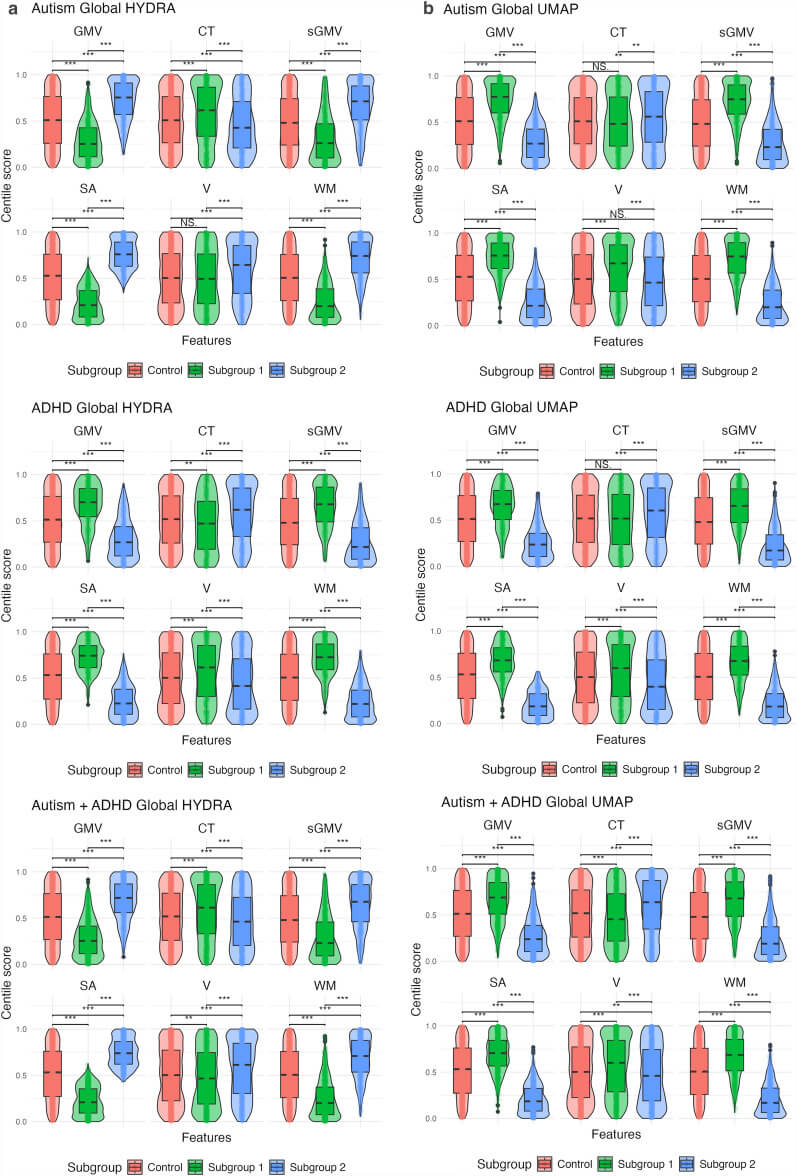
A June 2025 neuroimaging study examining brain structure patterns across individuals with autism, ADHD, and combined diagnoses, published in Molecular Autism by Pecci-Terroba and colleagues applies population modelling to cluster participants based on centile scores for cortical thickness, surface area, and grey matter volume, using HYDRA—a semi-supervised machine learning algorithm that identifies subgroups based on differences from neurotypical controls—and compares its performance against traditional clustering methods.
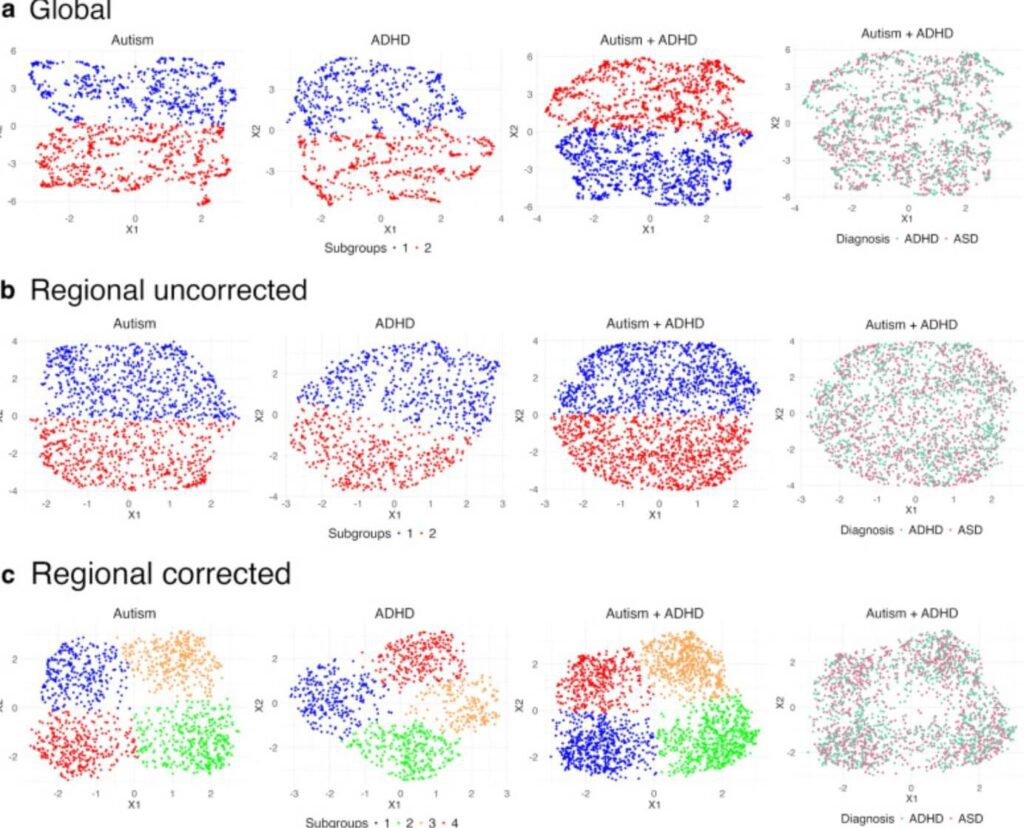
The image depicts scatter plots showing brain imaging data across individuals with autism, ADHD, and combined autism + ADHD diagnoses, using UMAP (Uniform Manifold Approximation and Projection) to visualize complex neurological patterns. The plots demonstrate how different analytical approaches—global features, regional uncorrected features, and regional corrected features—reveal varying degrees of overlap and distinction between diagnostic categories.
For educators, this visualiaation carries several implications that reach beyond the technical mechanics of brain imaging into the daily architecture of classroom practice, accommodation design, and the fundamental assumptions that structure how schools understand and respond to neurodivergent children.
The collapse of categorical thinking
The overlapping clusters in these plots reveal what many educators already observe in practice but what educational systems often refuse to accommodate: autism and ADHD exist along continuums rather than as discrete, separable conditions, and the co-occurrence of both diagnoses produces neurological profiles that blend rather than stack. When regional correction is applied—accounting for the specific brain structures involved—four distinct subgroups emerge even within what appears initially as unified diagnostic categories. This finding dismantles the assumption that a single accommodation strategy, a single behavioural intervention, or a single set of “autism supports” or “ADHD supports” can adequately serve all students carrying those diagnostic labels.
Educators working within rigid categorical frameworks—where students are sorted into autism programs versus ADHD support tracks, where IEP goals are generated from diagnosis-specific templates, where professional development trains teachers to recognise “the autistic student” or “the ADHD student” as though these were monolithic archetypes—encounter immediate tension when faced with students whose neurological profiles refuse such clean categorisation. The child who is both autistic and ADHD does not simply require two separate sets of interventions applied in parallel; the interaction between autism and ADHD creates distinct support needs that emerge from the combination itself, needs that categorical thinking cannot anticipate or address.
-

Neural evidence exposes the steep cost of sacrificing vulnerable children to punitive myths
Neural evidence from Altered Neural Responses to Punishment Learning in Conduct Disorder offers a precise account of how punitive school discipline collides with the neurodevelopmental profiles of vulnerable children, because the study shows that punishment learning relies on the anterior insula’s capacity to transform discomfort…
The inadequacy of diagnosis as pedagogy
These plots also expose the dangerous reduction that occurs when diagnosis becomes the primary organising principle for educational planning. Even within the “autism only” or “ADHD only” groups, the scatter plots show substantial internal variation; individuals cluster in different regions of the dimensional space, suggesting that people carrying the same diagnostic label possess meaningfully different neurological profiles. When educators rely on diagnosis as the primary information source for understanding a student’s learning needs, they risk applying generic, diagnosis-driven strategies to children whose actual neurological architecture requires something else entirely.
The educational system’s insistence on diagnosis-first planning—where access to support hinges on obtaining a formal diagnosis, where accommodations are justified through diagnostic criteria rather than observed need, where teachers are trained to implement “evidence-based practices for autism” as though autism itself were the sufficient description—creates a structural mismatch between what students require and what schools provide. A student appearing in the upper-right cluster of the “autism only” plot and a student appearing in the lower-left cluster carry the same diagnostic label but may need radically different sensory environments, instructional pacing, communication supports, and emotional regulation scaffolding.
-

Why the evolving understanding of childhood terrifies systems built on scarcity
Children now arrive at school shaped by homes that honour physiology over performance, autonomy over obedience, and co-regulation over fear, and this shift grows from a decade of relational neuroscience, trauma literacy, sensory understanding, and disability justice that families have absorbed far more…
The tyranny of normativity in measurement
The progression from “regional uncorrected” to “regional corrected” data reveals how analytical choices—which brain regions to examine, how to account for variation, what features to foreground—shape the patterns that emerge and, by extension, the conclusions drawn about difference and similarity. In educational contexts, this methodological reality translates into a persistent question: what counts as the baseline against which neurodivergent students are measured, and who determines that baseline?
Schools routinely assess neurodivergent students against neurotypical developmental trajectories, neurotypical attention spans, neurotypical social reciprocity patterns, neurotypical sensory thresholds, and neurotypical emotional regulation timelines. When students deviate from these norms, their differences are pathologised, targeted for intervention, and framed as deficits requiring correction rather than as variations requiring accommodation. The “corrected” analysis in these plots suggests that accounting for neurological structure—recognising the material reality of differently organised brains—reveals subgroup distinctions that remain invisible when data is analysed without such correction. Similarly, when educators fail to adjust their expectations, their assessments, and their pedagogical approaches to account for the structural differences in how neurodivergent students process information, regulate attention, manage sensory input, and navigate social demands, they misidentify student need as student failure.
The obligation to individualise beyond diagnosis
If these plots demonstrate anything, they demonstrate the insufficiency of diagnosis alone as the basis for educational planning. The four subgroups that emerge in the regionally corrected analysis for autism + ADHD indicate that even within this combined diagnostic category, meaningful neurological heterogeneity persists. For educators, this finding reinforces the necessity of individualised assessment, individualised accommodation design, and individualised instructional planning—processes that observe the specific child in front of them rather than inferring need from diagnostic label.
The tension here lies in the fact that schools are not structurally designed to individualise at scale. Individualized Education Programs (IEPs) are theoretically individualized but frequently consist of template goals, diagnosis-driven accommodations, and standardized behaviour plans applied across multiple students. The resource constraints, time limitations, and staffing ratios that characterize public education create systemic pressure to categorize, to generalize, and to apply one-size-fits-most solutions. The neurological reality captured in these plots insists that such generalization produces harm—that students sorted into the wrong subgroup, students whose specific neurological profile is misread through the lens of diagnostic stereotype, students whose overlap between autism and ADHD is treated as comorbidity rather than interaction, will be underserved, misunderstood, and subjected to interventions that worsen rather than support their functioning.
The violence of averaged outcomes
Research that measures intervention effectiveness by averaging outcomes across diagnostic groups obscures the reality that interventions effective for one subgroup may be neutral or harmful for another. When schools implement “evidence-based practices” derived from such averaged research, they risk applying interventions that work for some students while actively harming others, all while believing they are following best practices. A sensory intervention designed for one autism subgroup may overwhelm students whose sensory profiles differ; a behavioural strategy effective for one ADHD subgroup may escalate distress in students whose executive function challenges manifest differently.
Educators tasked with implementing these evidence-based practices often lack access to the subgroup-level data that would allow them to discern which students are likely to benefit and which are likely to be harmed. The guidance they receive—”use visual schedules for autistic students,” “provide movement breaks for ADHD students,” “implement token economies for students with behavioural challenges”—flattens the neurological heterogeneity these plots reveal, treating intervention as a matter of matching diagnosis to protocol rather than observing student response and adjusting accordingly.
The imperative of trust over assessment
These visualizations also carry an epistemological lesson: the patterns that matter most are often invisible until the right analytical lens is applied, and determining the right lens requires making choices about what to measure, how to correct for confounding variables, and which dimensions to prioritize. In educational contexts, this translates into the recognition that teachers cannot always see the neurological mechanisms driving student behaviour, but they can observe the behaviour itself and respond with curiosity rather than correction.
When a student’s distress, disengagement, or dysregulation is met with punitive response—when the teacher assumes the student is choosing defiance rather than experiencing overwhelm, when the school interprets the behaviour as manipulative rather than communicative, when the system demands compliance before offering support—the educator has chosen the wrong analytical lens. The regionally corrected plots suggest that accounting for underlying structure reveals meaningful distinctions; similarly, accounting for the structural reality of neurodivergent nervous systems—the sensory processing differences, the executive function variations, the interoceptive challenges, the demand avoidance profiles—reveals that behaviours often interpreted as volitional are in fact neurological.
The moral stakes of categorical refusal
Ultimately, these plots argue against the categorical thinking that structures so much of educational practice, diagnostic medicine, and disability policy. The overlap, the internal heterogeneity, the subgroup distinctions that emerge only with careful analysis—all of this insists that neurodivergence cannot be understood through the binary logics of presence or absence, the neat boundaries of DSM categories, or the assumption that diagnosis provides sufficient information for planning.
For educators, this means the work requires more than learning the characteristics of autism or the symptoms of ADHD; it requires learning to observe the specific student, to attend to their specific needs, to design accommodations responsive to their specific neurological profile, and to refuse the seductive efficiency of categorical generalisation. The plots reveal what individualised practice demands: that diagnosis is the beginning of understanding, never the end.
-

Rot at the root: Why POPARD must be dismantled from the top down
When I first objected to the strategies POPARD proposed, I tried—truly—to assume good intent: that if I just gave them the right information, the clearest language, the most generous interpretation of their mandate, they would course-correct and stop pushing reward charts onto an…