In the previous essay, I examined neuroimaging research demonstrating that autism and ADHD are not internally homogeneous diagnostic categories but rather contain multiple neurologically distinct subgroups, often with opposite patterns of brain structure alterations relative to controls. The Pecci-Terroba study reveals what categorical intervention logic refuses to accommodate: diagnosis alone cannot determine whether a specific intervention will be effective for a specific child, students carrying the same diagnostic label may belong to entirely different neurological subgroups requiring different supports, and the assumption that evidence-based practice means applying the same protocols to all students with the same diagnosis collapses under even minimal scrutiny of the heterogeneity literature.
-
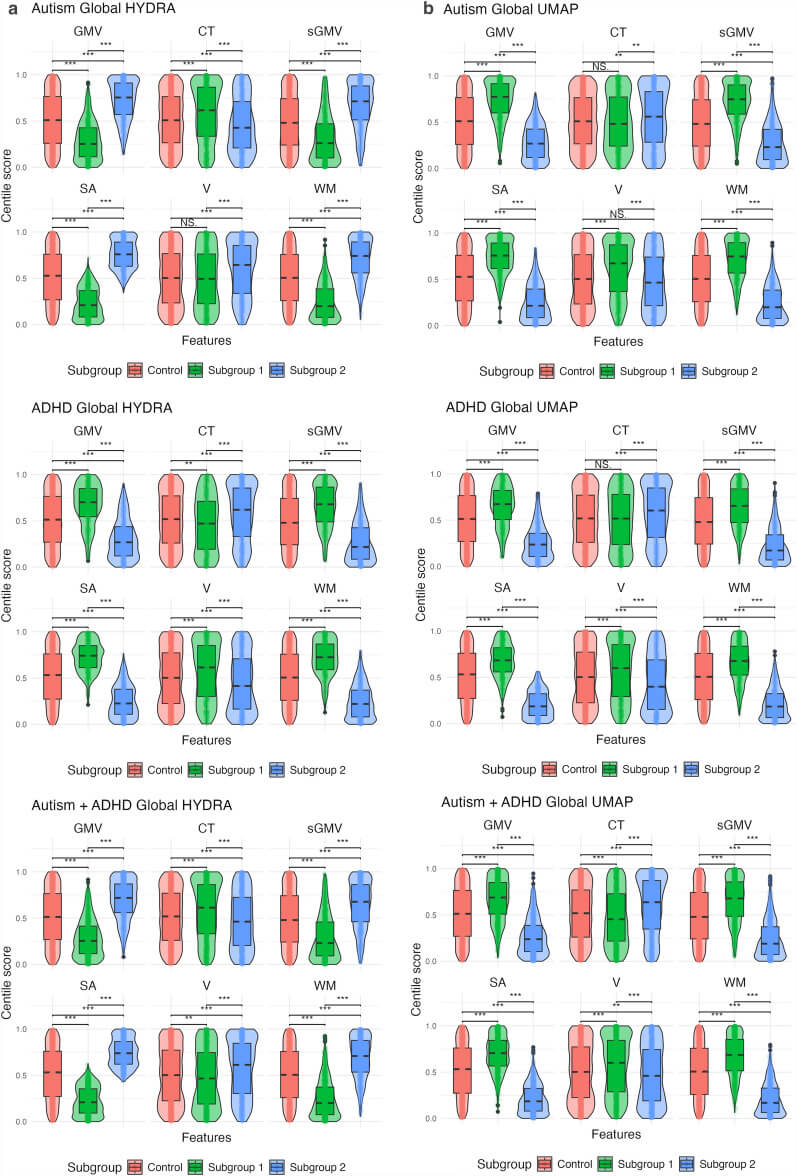
Subgrouping autism and ADHD based on structural MRI population modelling centiles
A June 2025 neuroimaging study examining brain structure patterns across individuals with autism, ADHD, and combined diagnoses, published in Molecular Autism by Pecci-Terroba and colleagues applies population modelling to cluster participants based on centile scores for cortical thickness, surface area, and grey matter…
This reality—that autism contains subgroups, that those subgroups may respond differently or oppositely to the same intervention, that individualised assessment matters more than diagnostic label—has immediate implications for how provincial bodies educate educators, how schools design intervention, and whether parental expertise receives recognition or dismissal when parents insist that categorical approaches will harm their specific child.
When I told POPARD—the provincial body tasked with educating British Columbia educators about autism—that implementing sticker charts for my son would be contraindicated given him PDA profile, they dismissed my concerns on two grounds: first, that PDA is not a real diagnosis and therefore my observations about demand avoidance carried no legitimate weight, and second, that sticker charts constitute evidence-based practice for autistic children and therefore should be implemented regardless of my objections. Both positions reflect the categorical thinking that heterogeneity research dismantles, the institutional refusal to recognize subgroup variation, and the systemic devaluation of parental knowledge when that knowledge challenges the convenience of one-size-fits-most intervention.
What follows is an account of how POPARD’s dismissal of my expertise—their insistence on categorical intervention despite individualised evidence of harm, their denial of PDA as a gatekeeping strategy, their misapplication of evidence-based practice to justify protocols contraindicated for my son’s specific neurological profile—exemplifies precisely the failure mode that studies like Pecci-Terroba’s expose. I was right, POPARD was wrong, and the neurological data confirms what I already knew from sustained observation of the child they claimed to be supporting through their categorical expertise.
-

Rot at the root: Why POPARD must be dismantled from the top down
When I first objected to the strategies POPARD proposed, I tried—truly—to assume good intent: that if I just gave them the right information, the clearest language, the most generous interpretation of their mandate, they would course-correct and stop pushing reward charts onto an…
The collapse of their categorical logic
POPARD’s position rested on a fundamental misunderstanding of what evidence-based practice requires in the context of neurodevelopmental heterogeneity. When research demonstrates that token economy systems produce positive outcomes for some autistic children, that finding does not establish that such systems will be effective for all autistic children, and it certainly does not establish efficacy for autistic children who also have ADHD, who present with PDA profiles, or who belong to neurological subgroups characterized by demand avoidance, executive function differences, or reward processing variations that make contingency-based systems actively harmful.
The neuroimaging data reveals what I was arguing based on clinical observation: the category “autism” contains multiple distinct subgroups with opposite patterns of neurological organisation. Some autistic individuals show increased cortical thickness in regions associated with reward processing and executive function; others show decreased thickness in those same regions. Some show heightened connectivity in circuits governing motivation and goal-directed behaviour; others show reduced connectivity. The intervention that supports one subgroup—external reward systems, structured behavioural contingencies, token economies—actively harms another subgroup by introducing demand, overwhelming executive function capacity, and triggering autonomic dysregulation through the coercive pressure embedded in contingency-based systems.
I presented evidence that sticker charts would be contraindicated for my son: evidence grounded in him specific PDA profile, him observable responses to demand, him documented distress when subjected to contingency-based systems. POPARD dismissed that evidence in favour of categorical thinking, prioritising the diagnostic label over the actual child, invoking “evidence-based practice” while ignoring the evidence I provided about my specific child’s neurological reality.
Their denial of PDA as gatekeeping strategy
POPARD’s insistence that PDA lacks legitimacy because it lacks formal diagnostic recognition functioned as rhetorical strategy for dismissing my expertise and refusing accommodation. Whether PDA appears in the DSM is irrelevant to the question of whether my son experiences demand avoidance, whether that demand avoidance produces genuine distress, and whether interventions designed to increase compliance through external reinforcement will exacerbate rather than support him functioning. The refusal to recognise PDA as legitimate serves institutional interests—it allows provincial bodies and schools to deny accommodations, to insist on compliance-based interventions, and to frame my resistance as unfounded rather than as informed advocacy grounded in sustained observation.
The heterogeneity revealed in studies like Pecci-Terroba’s supports the clinical reality of PDA even in the absence of formal diagnostic codification. If autism contains multiple neurologically distinct subgroups, and if those subgroups require different intervention approaches, then the existence of a subgroup characterised by pathological demand avoidance, autonomic overwhelm in response to perceived control, and distress triggered by contingency-based systems is entirely consistent with the broader picture of autistic heterogeneity. The fact that this profile has not yet been formalised in diagnostic manuals reflects the slowness of diagnostic nosology to catch up with clinical and neurological reality, not the absence of the phenomenon itself.
POPARD’s position—that my son’s profile lacks legitimacy because it challenges recognised categories—privileges institutional authority over parental observation, diagnostic manuals over lived experience, and categorical convenience over individualised response. The logic is circular: my son’s profile is dismissed because it does not fit recognised categories, and recognition is withheld because the profile challenges the categorical thinking that structures institutional practice.
The violence of their misapplied evidence
When POPARD insisted that sticker charts were evidence-based and therefore appropriate for my son, they committed a specific form of epistemic violence: they used the language of science to justify an intervention that the actual scientific evidence—evidence accounting for heterogeneity, subgroup variation, and PDA profiles—suggests would cause harm. The averaged outcomes supporting token economies do not disaggregate by subgroup, do not examine differential response among children with PDA characteristics, and do not account for the possibility that interventions effective for some autistic children are actively harmful for others.
My resistance to sticker charts was grounded in evidence: evidence from my observation of my son’s distress, evidence from the PDA literature describing autonomic dysregulation in response to demand, evidence from my understanding of him specific neurological profile and the way reward-based systems introduce coercive pressure that he experiences as intolerable. POPARD’s dismissal of that evidence in favour of categorical application of “evidence-based practice” demonstrates the gap between what research actually supports and what institutions claim research supports.
The Pecci-Terroba study provides the neurological scaffolding for the clinical argument I was already making: if autism contains subgroups with opposite patterns of brain organisation, if those subgroups require different interventions, and if applying the wrong intervention to the wrong subgroup produces harm rather than benefit, then the insistence on categorical intervention—sticker charts for all autistic students because sticker charts are “evidence-based for autism”—constitutes malpractice. Evidence-based practice requires identifying which subgroup a child belongs to and selecting interventions appropriate for that subgroup, not applying averaged intervention protocols without attention to individual variation.
-

The high stakes of understanding PDA
Pathological Demand Avoidance (PDA) might sound like just another clinical term, but for many families it represents a daily struggle that is anything but trivial. PDA is a profile on the autism spectrum characterised by an extreme, anxiety-driven avoidance of everyday demands, even those the child wants to…
The institutional refusal I was confronting
POPARD’s response exposed a structural gap between what neurodevelopmental science shows and what educational institutions are willing to accommodate. Recognising heterogeneity, individualising intervention, and abandoning categorical thinking demand more resources, expertise, and epistemic humility than institutions are prepared to offer. It is easier to mandate uniform “evidence-based” practices, dismiss parental concerns as resistance, and deny the legitimacy of PDA than to redesign systems around genuine neurological variation.
Although POPARD claims to educate educators about autism, its mandate is constrained by scalability and existing resource limits. The result is guidance that flattens complexity, treats diagnosis as sufficient information, and promotes evidence-based practices without interrogating whom that evidence actually serves.
What I knew that they refused to hear
Studies such as Pecci-Terroba’s validate what I was arguing all along: my observations of my son carry more weight than averaged research findings, and my insistence on intervention grounded in his specific neurological profile reflects scientific literacy, not parental overreach. The data confirm that categorical, diagnosis-driven interventions ignore subgroup variation and that evidence supporting sticker charts for some autistic children does not justify their use for all—certainly not for my son.
POPARD’s dismissal of my expertise reflects a broader institutional devaluation of parental knowledge and lived observation. When I said sticker charts would harm my son, I was making an evidence-consistent claim grounded in his PDA profile. Their response was to invoke “evidence-based practice” while ignoring heterogeneity, dismiss PDA as illegitimate, and insist on interventions known to exacerbate demand avoidance. The neurological data simply confirms what I already knew: my son belongs to a subgroup for whom their prescribed intervention is contraindicated, and their refusal to individualise represents a failure to practice in accordance with the science they claim to follow.
-

Shut it down: Why POPARD cannot be trusted to support neurodivergent children
We asked for help.We got a behaviour chart. We invited experts into our child’s life, hoping they would help school staff understand his anxiety, his trauma responses, his fiercely sensitive nervous system. We asked for relational strategies grounded in respect and attunement. We…